Having done numerous surgical operations on palate and uvula, and with an aim to avoid velopharyngeal insufficiency and improve functional results of earlier techniques, I have developed new technique: arco-palato-uvular flap (APUF). This kind of surgical intervention is improvement in previously used uvulopalatinal flap(1). The method is less invasive with possibility for subsequent correction. Preliminary results of such surgical intervention have been reported at the symposium devoted to loud snoring (Belgrade, 2004, 13th congress of Balcan Military Medical Committee, Kusadasi, Turkey, June 2008). At the meeting, the method was accepted as an exceptional innovation. |
This kind of surgical intervention, done in general anesthesia, is effective. Consolidation and stabilization of rear palatal arch, free and lowered edge of soft palate and uvula, and simultaneous enlarging of oropharyngal airway represent the goal of such intervention. Final appearance of this intervention resembles the one obtained by uvulopalatopharyngoplastics, except that uvula, palate arches and free palate edge are not excluded but incorporated in local region in the shape of flap. |
 |
 |
| Local finding in the throat that represents optimal conditions for arco-palato-uvular flap application Rear palate arches are wide and, rugged, palate thinned, downcast, uvula short, tonsils earlier excluded |
Uvula’s length is reduced in width and thickness, and shaped according to the need that is requested by flap Mucous membrane of free edge of posterior pillars and soft palate are made vulnerable Tissue of rear palate arches, approximately 0,5cm in length is being cut by horizontal incision (above tongue basis) |
Aim of the work:
Conditions for intervention:
Local finding in the throat that represents optimal conditions for arco-palato-uvular flap application Rear palate arches are wide and, rugged, palate thinned, downcast, uvula short, tonsils earlier excluded Criteria for surgical treatment (Dr. Vukoje Method):
|
 |
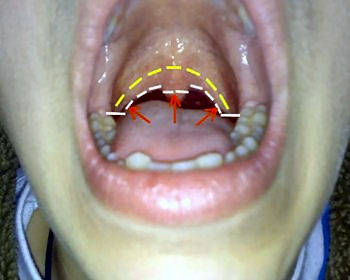 |
| Positioned away 0.5cm from free edge, incision is made at the mucous membrane of the posterior pillars and soft palate Incision starts above the tongue basis, runs vertically and follows free edge of soft palate, and finally joins the same incision that started from the other side of the arch |
Arco-palato-uvular flap is being formed and bended lateral and towards hard palate, and fixed by adequate number of stitches (VicrylTM, Johnson & Johnson Ethicon, 4-0 sutures) |
Patiens and methods Twentyseven non-apneic snorers did not repeat Apnea Graph. A VAS scale (amount of snoring noise during sleep) that was used, required the subject, along with his or her bed partner, to assess snoring levels.The pretreatment scale was compared with the final posttreatment scale.The scale ranged from 0(no snoring noise) to 10(extreme noise - bed partner leaves the room). Post-operative snoring loudness was documented for 1-2 years period. All patients were asked to complete the Epworth Sleepness Scale and VAS to obtain information regarding “devastating noise”. During the follow-up period the patients were seen by the surgeon after one, six and twelve weeks. All patients had body mass index (BMI) less than 30. None of the patients had previous surgery for snoring. Preoperatively, clinical assessment scores were as follows VAS (8,6-+1,0), ESS (l0,0-+3,0) postoperatively VAS (2,3+-1,5) ESS (4,0+-1,). Snoring was without improvement in 2 patients (8,4%) In patients with mild apnea AHI before surgery was (11,58 +-3,58) after surgery AHI (4,75+-2,92). Statistical analysis revealed significant reduction for all variables(P < 0001). In no case did we observe any evidence of postoperative scarring, fibrosis, or any other clinically significant side effect. One patient complained of a mild degree of mouth dryness and two reported a globus sensation. Discussion These complications no noted with APUF.Recently developments have resulted in more targeted procedures to stiffen the palate and cause less surgical trauma for patients.These procedures include radiofrequency and injection sclerotherapy of the palate .However,these regimens require more than one treatment for optimal palatal stiffening and can cause mucosal breakdown and fistulas. After tonsillectomy the posterior pillars and palatal muscle stratum become insufficiency, the stiffening method and palate sclerosation is, in thinned and atrophy soft palate and arches, contraindicated. Insertion method of palatal implants could not be applied because it requires strict indications for application (5, 6) - hypertrophy of soft palate and short uvula that in those cases did not exist. Long term stable results of APUF and higher percentage of success are achieved comparing to other surgical interventions on that segment (3, 7, 8) Method does not need to compromise CPAP usage and maximum pressure that patient can tolerate. On the other hand, one of the UPPP complications is nasopharyngeal stenosis (4, 9, 12) which compromise use of CPAP.
Advantage of UPPP lies in its wider indicative region than of the APUF. Both interventions widen airway and are in need of total anasthesia. Comparing scope of work between UPPP and APUF we see that UPPP does not depend on anatomical structure of throat and it reduces free palate edge and removes uvula and tonsils (11,14,). Arco-palato-uvular flap requests strict indications. If these indicatios are respected, success can be expected.Several years of follow up results have proven the APUF to be a well tolerated,efficient and recomendable for the defined target group. Conclusions
|

